
Annals of Robotic Surgery
Totally Robotic Esophagectomy: The Largest Series
Abstract
Introduction: The high morbidity and mortality after the conventional esophagectomy lead to the need for innovation in the field of minimal access esophagectomy, initially thoracoscopy and now is the era of Robotics. This paper presents the results of totally robotic esophagectomy in a series of 162 patients.
Materials and Methods: This is a retrospective study of 162 patients undergoing totally robotic esophagectomy for carcinoma esophagus in a single institute for a period of 4 yrs from January 2013 to January 2016.
Results: Variables such as age, gender, site, and histology, and operative time, amount of blood loss, ICU stay and number of lymph nodes harvested are taken into consideration in this study. The overall operative time ranges from 200 min to 420 min average being 292.4 min. The mean number of lymph nodes harvested was 42.36 (range 38-48) which can be considered to be highest among all as per our knowledge till date. Mean ICU stay was 2.3 days. Median follow-up period of 18 months showed 145 (89.5%) patients alive with disease free stage.
Conclusion: Robotic esophagectomy clearly shows an advantage in the aspects of accessibility and higher yield of lymph nodal clearance apart from reduced morbidity and mortality.
Introduction
Esophageal carcinoma ranks eight among the cancers worldwide. According to global cancer statistics 2018, there are 572,034 of new cases of esophageal cancers and 508,585 estimated deaths in a year [1]. Its high incidence and mortality lead to multidisciplinary approach in which surgery remains the main cornerstone with curative intent [2]. The high morbidity and mortality after the conventional esophagectomy lead to the need for innovation in the field of minimal access esophagectomy, initially thoracoscopy and now is the era of robotics. Robotics takes a special place in the domain of thorax due to its higher degree of arm rotation and accessibility in the closed space. This paper shows the results of totally robotic esophagectomy in a series of 162 patients.
Materials and Methods
This is a retrospective study of 162 patients undergoing totally robotic esophagectomy for carcinoma esophagus in a single institute for a period of 3 yrs from January 2013 to January 2016.
Pre OP work up
All the patients underwent a through clinical examination followed by required investigations for surgical fitness and imaging modalities for staging the tumour. Clear consent of the patient was taken to use their data and footages if needed for clinical research and academic use. Consent was taken from each and every patient regarding the possibility of conversion to either thoracoscopic or open technique if the situation demands.
Patient selection
The study population included patients with carcinoma at the middle and lower esophagus. Both the histological types-squamous and adenocarcinoma variants are included. Patients with severe co-morbid conditions, those with carcinoma at the upper esophagus and those with stage IV disease were excluded from the study.


Operative technique
Position: The patient was placed in prone position for esophageal mobilization (falls anteriorly and simplifies dissection) and supine position for stomach mobilization and cervical anastomosis.
Port placement: The robotic cart is positioned to the left side of the patient (prone position) for esophageal mobilization. Port positions are as follows:
- 12 mm camera port- 1 finger breadth below and posterior to inferior scapular angle in the 5th to 6th intercoastal space and pneumo-insufflation done.
- Two 8 mm arm ports- in a vertical line at a distance of 5 cm and in triangulation with the camera port in the 3rd and 8th intercoastal space respectively.
- 10 mm assistant port-between left working and camera port.
Mobilization of the esophagus is done, harvesting the pre tracheal, paratracheal, subcarinal, lower and middle mediastinal and recurrent laryngeal nodes of both the sides. Recurrent laryngeal nodes of the left side were approached by dissecting through the Aortopulmonary window (Jagdish Technique) (Figure 1). Usually, in most of the cases azygous vein was preserved but sacrificed (Figure 2) in few if required for better oncological clearance.
The robotic cart is positioned at the head end of the patient (supine position) for stomach mobilization. Port positions are as follows:
- 12 mm camera port- umbilical port.
- Two 8 mm arm ports- bilateral mid clavicular regions.
- 10 mm assistant port- right iliac fossa or left iliac fossa according to surgeons’ convenience (we choose right iliac fossa due to our ease in conduit preparation by endo staplers [ethicon]).
- 8 mm retractor port- right hypochondrial region for liver retraction.
Mobilization of the stomach done and harvesting of paraesophageal left and right gastric, splenic and hepatic artery nodes done. Gastric conduit was prepared based on right gastro epiploic artery intracorporeally using GI staplers (Ethicon- linear endo staplers).
Left supra clavicular incision is given; esophagus pulled into the wound and cut. Specimen retrieved through 5 cm incision in the abdomen. Stomach conduit is rail roaded into the neck and hand sewn esophagogastric anastomosis done. Prophylactic intercoastal drains placed bilaterally in all the patients and feeding jejunostomy done.
Post OP care
Post operatively patients were kept in ICU for an average of 3 to 4 days and then shifted to ward. The chest radiograph and complete blood picture was done in the early postoperative phase and later only if the patients is in distress or shows signs of any complications. Within 24 h the patient is ambulated and jejunostomy feeds started within 48 h. Oral feeds are started on 7th day after performing leak test and patients discharged home. Depending upon the nodal status patient is subjected for chemotherapy or radiotherapy or both.
Follow-up
All the patients are followed up for 3 complete years. It includes clinical examination, ultra sonography and chest radiograph every 3 months for the 1st year, followed by every 6 months for a period of 2 years.
Results
Variables such as age, gender, site, histology, and operative time, amount of blood loss, ICU stay and number of lymph nodes harvested are taken into consideration in this study. Out of 162 patients included 115 (70.9%) are males and 47 (29.1%) are females. The youngest patient was 23 yrs of age and the oldest being 81 yrs, majority among them lie between the ages of 50 to 70. Most commonly involved site was lower third of the esophagus and histological predominance was of squamous cell carcinoma accounting for 94 (58.4%) and 132 (81.4%) patients respectively of the study population.
The overall operative time of both the thoracic as well as the abdominal procedures with the time of docking and undocking included ranges from 200 min to 420 min; average being 292.4 min. At the initial phase of learning curve, the time taken was more but later we fastened with experience. Intra operative blood loss ranged from 100 ml to 300 ml, average being <170 ml which also improved with experience. The mean number of lymph nodes harvested was 42.36 (range 38-48) which can be considered to be highest among all as per our knowledge till date. There was not even a single conversion to either thoracoscopy or open techniques, 1 case was inoperable, and none showed positive circumferential margins.
The mean ICU stay was 2.3 days (range 2-5), 5 patients had post operatively respiratory complications, 2 patients required temporary ventilatory support and tracheostomy was done in 2 cases and so required prolonged ICU stay. Anastomotic leak was reported in 2 cases, one was managed conservatively other needed re exploration. Chyle leak was seen in 3 patients, all were managed conservatively. None of them had port site metastasis, 4 patients had recurrent palsy. Death occurred in 1 patient due to cardio pulmonary cause (non surgical related). We lost 4 patients for follow up, median follow-up period of 18 months showed 145 (89.5%) patients alive with disease free stage.
Discussion
Robotic esophagectomy, in this present era is making its place due to lower morbidity and mortality. Esophagectomy as such is a very skillful technique which requires lots of surgical expertise at the same time is associated with high rates of mortality and morbidity. Complications like massive bleeding, tracheal injuries, cardiac arrhythmias, incidental splenectomies, pulmonary complications and leaks were high in conventional techniques leading to higher hospital stay and higher rates of mortality [3]. Minimal invasive esophagectomy has come into existence in order to reduce the morbidity and mortality pertaining to open procedures and improve the quality of life [4]. The limitations of MIE such as 2D vision, fulcrum effect of the instruments, limited maneuverability, tremors and uncomfortable surgeons’ position has encouraged to increase access on the robot [5].
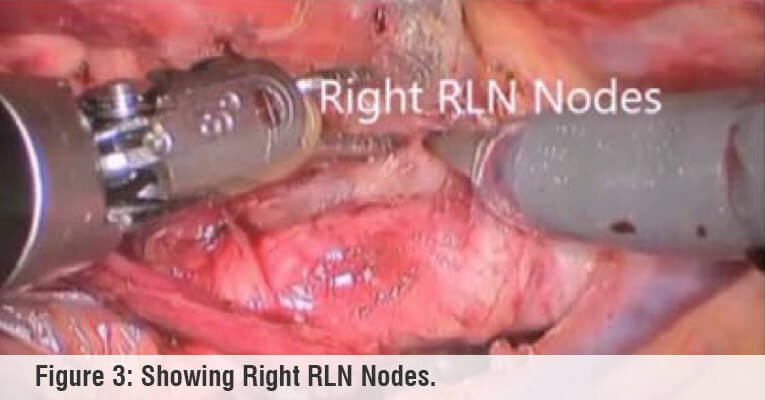
Due to harder learning curve and access to the robot, robotic esophagectomy has been delayed till the early part of this decade. The robot took advantage over other minimal invasive esophagectomy due to improved 3D vision which aids in precise dissections around vital structures like trachea, recurrent laryngeal nerve, aorta, pulmonary window, thoracic duct etc. The seven degrees of dexterity of the robotic arm improves access to the unaccessible sites and increased lymph nodal harvestment thus improving oncological clearance. Tremor free mobility added and edge for fine dissection and precision in marginal clearance thereby reducing the overall operating time. In our study overall operating time (292.4 min) is very less when compared to others like Park SY et al. [6] study. In our study we have harvested the paraesophageal, subcarinal, mediastinal, bilateral recurrent laryngeal lymph nodes (Figure 3) by accessing through the aortopulmonary window. There are studies showing reduced incidence of recurrent laryngeal nerve injury (Suda et al. [7]) and increase lymph nodal yield (Park et al. [8]) by robotic approach when compared to other minimal invasive approaches.
Conclusion
Robotic esophagectomy clearly shows an advantage in the aspects of accessibility and higher yield of lymph nodal clearance apart from reduced morbidity and mortality. Difficulty in the learning curve should be surpassed to reap the benefits of this approach both for the patients as well as the operating surgeon.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424.
- Mariette C, Piessen G, Triboulet JP. Therapeutic strategies in oesophageal carcinoma, role of surgery and other modalities. Lancet Oncol. 2007;8(6):545-53.
- Katariya K, Harvey JC, Pina E, Beattie EJ. Complications of transhiatal esophagectomy. J Surg Oncol. 1994;57(3):157-63.
- Zheng Ma, Huijun Niu, Taiqian Gong. Thoracoscopic and laparoscopic radical esophagectomy with lateral-prone position. J Thorac Dis. 2014;6(2):156-60.
- Marco Taurchini, Antonello Cuttitta. Minimally invasive and robotic esophagectomy: state of the art. J Vis Surg. 2017;3:125.
- Park SY, Kim DJ, Yu WS, Jung HS. Robotic-assisted thoracoscopic esophagectomy with extensive mediastinal lymphadenectomy: experience with 114 consecutive patients with intrathoracic esophageal cancer. Dis Esophagus. 2016;29(4):326-32.
- Suda K, Ishida Y, Kawamura Y, Inaba K, Kanaya S, Teramukai S, et al. Robot‐assisted thoracoscopic lymphadenectomy along the left recurrent laryngeal nerve for esophageal squamous cell carcinoma in the prone position: technical report and short‐term outcomes. World J Surg. 2012;36(7):1608-16.
- Park S, Hwang Y, Lee HJ, Park IK, Kim YT, Kang CH. Comparison of robot‐assisted esophagectomy and thoracoscopic esophagectomy in esophageal squamous cell carcinoma. J Thorac Dis. 2016;8(10):2853-61.





 Appointment
Appointment Second Opinion
Second Opinion WhatsApp
WhatsApp Call
Call More
More





{kind=link}