
A Challenging Case of Left Leg DVT in A Young Girl

Background
9 yrs, Female, Software employee presented with pain in left leg and swelling in left leg upto thighs since 10 days .Past h/o PCOD, Cholecystectomy (2014), LSCS (2015), h/o taking OC pills since 8 months.
Examination And Investigations
O/E: HR: 90bpm, BP: 80 mmHg Sys
Left LL Swollen upto thigh with bluish discolouration
CVS/RS : Normal
ECG: SR, No ST-T changes
2D Echo: RA/RV normal, No e/o PTE. Normal LV/RV function
Lab: Ok
Left LL venous doppler: large thrombus from Left CIV to popliteal V — s/o Ileo-femoral DVT
CT Venogram: Acute DVT involving Left CIVein, Ex Iliac Vein, CFVein, SFV, popliteal vein,
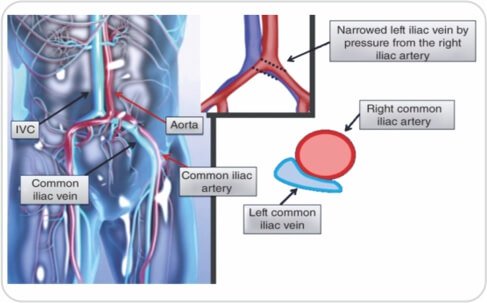
Left CIV seen passing between Right CIA and vertebral body and is narrowed
s/o MAY-THURNER Syndrome


Treatment
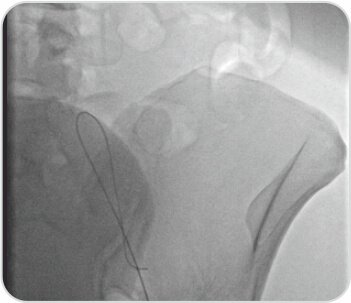
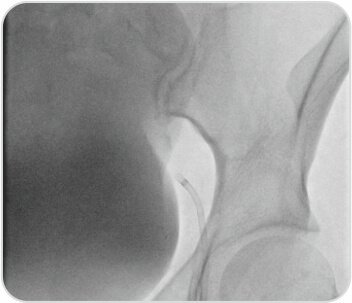
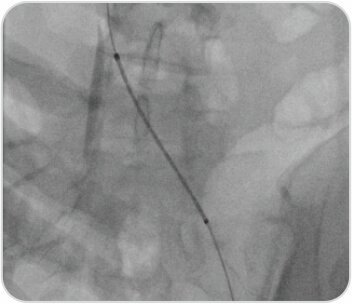
Plan: IVC filter, Mechanical Thrombusuction, Catheter Directed Thrombolysis, check Venogram. Venoplasty and Stenting of CIV.Accessed the popliteal vein under U.S. guidance.
A 6-F sheath was inserted. Terumo wire crossed, Angio showed large thrombus burden, occlusion of Ileo-femoral venous system.
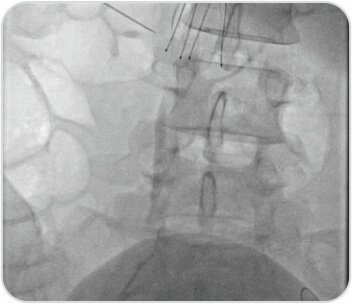
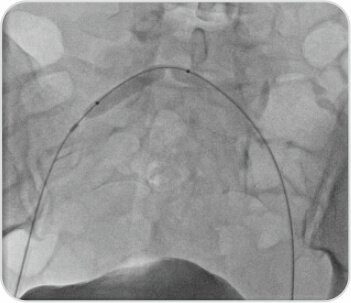
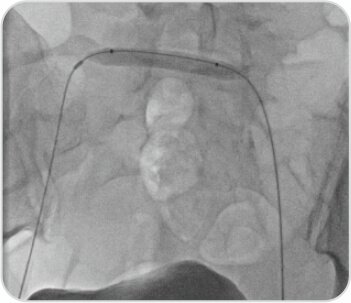
IVC filter: (7F, cook): A 6-F sheath was placed into the right common femoral vein; Rt iliac venography and cavogram was done followed by deployment of retrievable IVC filter just below renal vein

Mechanical Thrombusuction : Negative pressure to the catheter
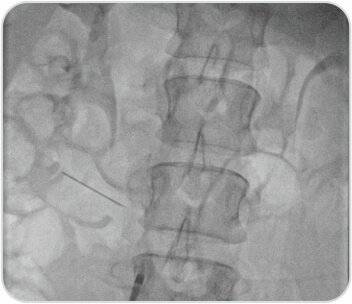
CDT: Multiside port catheter 5f: Urokinase infusion using (multi-side port catheter infusion set, cook ). 5lac units bolus f/b 50000 units/hr of Urokinase injected through infusion catheter, and 8f sheath was also connected to Heparin infusion pump with a dose of 1000 units /hour, Lysis progress was checked by venography at 8 hours interval. Total Lysis duration was 16 hours. F sheath was placed into left common femoral vein, check venogram was done, partial resolution of thrombus and residual significant occlusion of iliac vein was observed .
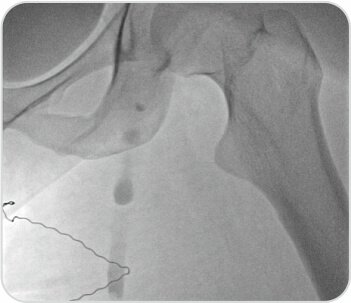
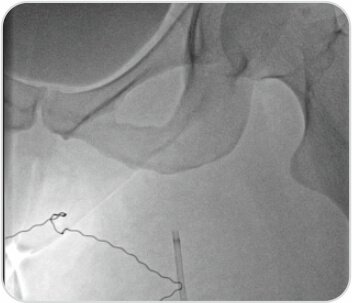
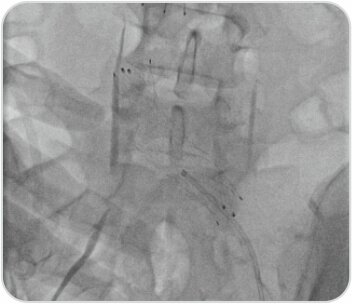
Lesion was very difficult to cross, multiple attempts made, (long sheath, Vert catheter, Rubicon catheter) finally Terumo wire could be negotiated into Rt CIV. Wire snared from Rt. CFV.

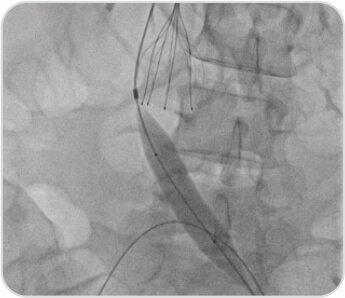
F/B 7 ×40 mm (Conquest PTA balloon)
was crossed, predilatation done. Tight Lesion
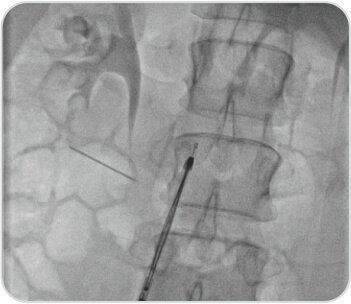
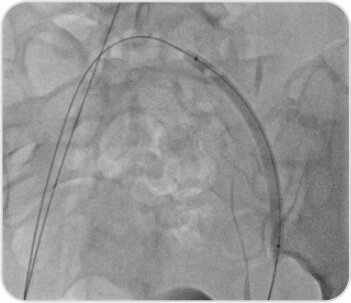
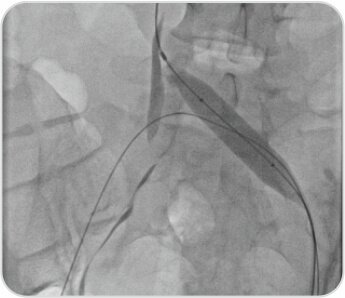
Venoplasty with , multiple balloon dilatation were done starting by 2.5×80 mm. PTA balloon Sheath in left groin changed to 11F , 12 × 40 mmAtlasPTAballoonat24atm.Adequate Dilatation at bifurcation into IVCA post-angioplasty venogram demonstrated a widely patent stent and good contrast flow through the stent into the inferior vena cava, without filling of the cross-pelvic collaterals.
Discussion And Conclusion
A history of persistent left lower extremity swelling with or without DVT in a woman between the 2nd and 4th decades, without an obvious cause of hypercoagulation, highly suggestive of May-Thurner syndrome, this possibility should be assessed with CT and iliac venography.
If the patient has extensive thrombosis, to prevent limb loss, circulatory collapse, and death, it may be appropriate to consider: Pharmacomechanical thrombectomy. Catheter-directed thrombolysis (CDT) and Angioplasty and stenting of the iliac vein
Challenge in this case: difficult fibrotic lesion, requiring a lot of effort, multiple attempts to cross and predilate the lesion with serial balloons. Finally good result achieved.



 Appointment
Appointment Second Opinion
Second Opinion WhatsApp
WhatsApp Call
Call More
More





{kind=link}