
Primary angioplasty for Acute Myocardial infarction

Myocardial infarction, commonly known as a heart attack is the irreversible death of heart muscles due to ischemia (prolonged lack of oxygen). It is a medical emergency which usually occurs to obstructed blood flow due to blood clots.
Over the past decades, treatment for myocardial infarction has evolved considerably. Reported mortality rates have fallen as a result of early diagnosis and treatment, improved management of its complications. Most attention is given to restore antegrade coronary blood flow in the affected artery of the patient with evolving acute myocardial infarction. There are two ways to achieve this goal:
- Using thrombolytics to dissolve the clots and allow continuous blood flow
- Immediate coronary angiography followed by primary angioplasty
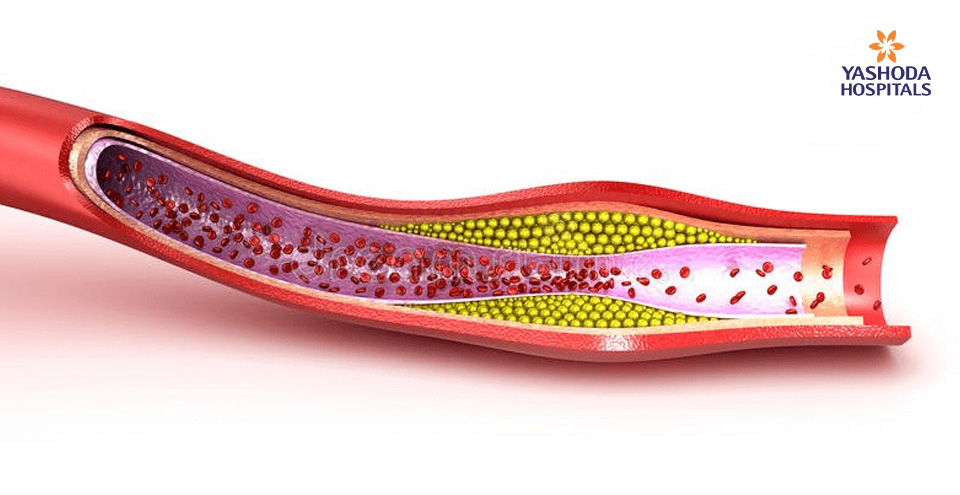
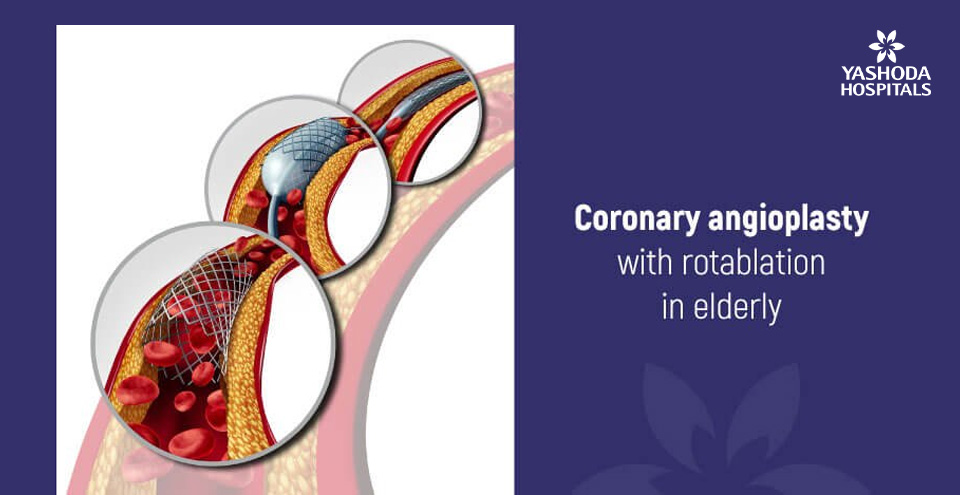
The formation of coronary thrombus on an atherosclerotic plaque, leading to a total or subtotal occlusion of the coronary artery, is the key event that causes acute ischemic syndromes as shown in the image below. Treatments that restore antegrade blood flow in the affected coronary artery are of paramount importance.

Patients with acute myocardial infarction need emergency treatment to unblock the coronary artery, such as
- Primary angioplasty
- A ‘clot-breaking’ medicine to dissolve the blood clot that is blocking the coronary artery. In this article, I will discuss the primary angioplasty, its indications, and advantages over thrombolysis.
Primary angioplasty without the use of thrombolytics was described in the year 1983. Primary angioplasty is a treatment to re-open a blocked coronary artery. When an angioplasty is used to re-open a coronary artery when someone is having acute myocardial infarction, it is called a primary angioplasty. Primary angioplasty should be performed as immediately as possible after the symptoms of a heart attack start. Successful primary angioplasty results in a reduction in time to first balloon inflation by 30–40 minutes.
Earlier diagnosis by electrocardiography in the ambulance or nearby hospital, rapid transportation to heart institutes where the 24×7 facility of interventional cardiology of the best available option should be the first priority.
The ambulance and paramedics work closely with the hospitals and doctors in their area to try to make sure that people with a suspected heart attack are taken to a hospital that can carry out a primary angioplasty. The patient can be shifted into the cath lab directly bypassing emergency room for the early treatment.
An overview of short-term results of comparisons of the two approaches has shown that, compared to thrombolysis, primary angioplasty results in a lower mortality (4.4% v 6.5%), translating into an absolute benefit of two lives saved per 100 patients treated with angioplasty compared with thrombolysis. The incidence of stroke was reported to reduce from 2.0% with thrombolysis to 0.7% with angioplasty. Primary angioplasty is more cost effective than for thrombolysis in several settings.

“The higher the risk of the patient, the greater the potential of primary angioplasty compared with thrombolysis”
After the development of safe and effective antiplatelet agents [blood thinners given to maintain the patency of stent], stenting has had a profound effect on the performance and results of primary angioplasty both in the acute phase and follow up. The use of drug-eluting stents are cost-effective by reducing the rate of restenosis, stent eligible patients have a reduced need for repeat hospitalization and procedures.

Primary angioplasty of a patient who presented with an acute inferior wall ST-elevation myocardial infarction is shown in the image above.
A: Coronary angiography showed proximal thrombotic occlusion (TIMI 0 flow) of the right coronary artery. The Left coronary artery was normal.
B: Predilatation with a balloon after thrombo-aspiration.
C: Establishment of flow in the right coronary artery with few thrombi and residual stenosis at the proximal segment.
D: Placement of the drug-eluting stent at the site of the lesion.
E: Final angiography showing brisk TIMI 3 flow in the right coronary with good distal myocardial blush score.
F: Red thrombus aspirated from culprit vessel – right coronary artery using thrombo-aspiration catheter
Candidates undergoing thrombolytic treatment may be recommended to undergo primary angioplasty as an alternative reperfusion therapy when there is no other option for reperfusion.
Based on the health status of the patient, doctors may decide to perform primary angioplasty:
- Patient shows signs of a large myocardial infarction and contraindications for thrombolytic treatment
- Patients with two or more high-risk factors:
- Age > 70 years
- Anterior wall myocardial infarction
- Heart rate > 100 beats/min
- Systolic blood pressure < 100 mm Hg
- Previous myocardial infarction
- Previous coronary artery bypass grafting
- Diabetes
- Patients eligible or not eligible for thrombolytic treatment, with one or fewer high-risk characteristics, but with signs of a large myocardial infarction.
The first hour after the onset of a heart attack is called the golden hour. Immediate access to heart care is important within this golden hour. Emergency Care at Yashoda Hospitals is an exclusive center that offers immediate treatment in an emergency with the highest level of care, round-the-clock. All our cardiologists, Emergency Medicine specialists, trauma surgeons, and support staffs are highly trained to deal with cases of heart attack for patients in need of prompt care.
The center offers day-and-night service with 24/7 access to modern operation theatres, imaging & diagnostic tools and fully stocked 24-hour pharmacies for immediate and accurate diagnosis of the patient’s condition.
About Author –
Dr. Pankaj Vinod Jariwala, Consultant Interventional Cardiologist, Yashoda Hospitals – Hyderabad
MD, DNB, DNB, MNAMS, FICPS, FACC.
Fellowship in Interventional Cardiology [ICPS, Paris, France]He has performed 5000+ percutaneous trans-luminal coronary Angioplasty & 10,000+ Coronary Angiograms and treated 500+ structural heart diseases (including congenital) with Percutaneous Balloon Mitral Valvuloplasty [PBMV] and other pediatric & adult cardiac interventions.
About Author

Dr. Pankaj Vinod Jariwala
MD, DNB (Cardiology)Consultant Interventional Cardiologist










 Appointment
Appointment Second Opinion
Second Opinion WhatsApp
WhatsApp Call
Call More
More





{kind=link}