Acoustic Neuroma – Important Things To Know About

At a glance:
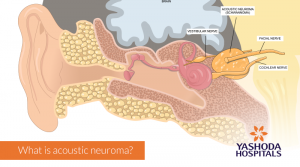
What is acoustic neuroma?
Acoustic neuromas are slow-growing, non-cancerous (benign) tumor of acoustic nerve found behind the ear, directly under the brain. The word acoustic neuroma means “neuroma” or tumor of the nerve of hearing i.e “acoustic” nerve. Acoustic neuromas are also known by the name Vestibular Schwannomas. This is so because they originate from a special type of cells called Schwann cells which cover the nerve cells in the body. Acoustic neuroma is usually slow-growing and generally does not show any tendency to spread to any distant part of the body. Since it is not cancerous. i.e it doesn’t spread to any other part, it is called a benign tumor.
The tumor grows near the brain stem that houses 12 cranial nerves. The nerves of the brain are called cranial nerves, which are 12 in number on each side and arranged in a specific sequence. The 8th cranial nerve is known as the acoustic or vestibulocochlear nerve. It connects the ear with the brain and is associated with the function of hearing and balance. An acoustic neuroma is a rare type of brain tumor that originates from the 8th nerve.
What are the causes of acoustic neuroma?
Even though the exact cause of an acoustic neuroma is uncertain, in some cases, it has been attributed to a rare underlying genetic disease, neurofibromatosis type 2 (NF2) that affects about 1 in 25,000 people. NF2 is associated with non-cancerous or benign tumors of the nervous system.
Acoustic neuroma in people with NF2 mostly occurs on the nerves of hearing on both i.e bilateral sides of the head. On the other hand, acoustic neuroma in case of people not suffering with NF2 is usually on one side i.e unilateral. People with NF2 are also more prone to developing tumors of the covering sheet of brain i.e membrane and the spinal cord, like glioblastoma.
What is acoustic neuroma?
How common is acoustic neuroma?
Developing in between 1 and 20 people per million population worldwide, acoustic neuromas are rare tumors. About 6 in 100 brain tumors are identified to be acoustic neuroma. This category of brain tumors is more commonly diagnosed in middle-aged adults and seen rarely in children. The tumor is more common in men as compared to women.
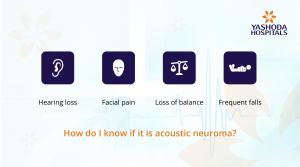
What are the symptoms of acoustic neuroma?
Acoustic neuroma symptoms may vary from case to case. In some cases, there may not be any symptoms. Acoustic neuroma symptoms even if present, usually develop slowly due to the slow-growing nature of the tumor.
Some of the commonly seen symptoms of an acoustic neuroma are:
- Hearing loss: Most people with acoustic neuroma report some degree of deafness. Hearing loss may be gradual and noticed only in one ear. The type of deafness that is caused due to acoustic neuroma is known as sensorineural deafness. It means that there is a damage to the acoustic nerve or the nerve for hearing.
- Tinnitus: With almost 7 in 10 people suffering from acoustic neuroma reporting it, tinnitus i.e “a ringing sound” in the ears is a common symptom of acoustic neuroma. Sometimes the sound may not be really “ringing like a bell”. Any kind of sound that maybe heard within the ear in absence of an external sound being made is termed tinnitus. Earwax, aging, ear infections and noise-induced hearing loss are some other causes of tinnitus.
- Vertigo: Sometimes described as dizziness, vertigo is the feeling of spinning. Some people incorrectly describe it as a fear of heights. It is actually the feeling of movement that occurs when a person stands still which may lead to the induced feeling of fright of falling down when standing at a height. Vertigo can be a symptom for many other diseases of the inner ear and even though nearly half of the people suffering from acoustic neuroma report it at some point of time, very few people report it as their first symptom.
- Impaired ability to balance the body, disorientation & increased risk of falling and injuries: Due to vertigo and effect on the middle ear and the nerve, people with acoustic neuroma often fail to maintain body balance while walking or standing up.
- Facial numbness, tingling or pain: A growing acoustic neuroma may create a pressure on other neighboring nerves, mostly the 5th, i.e trigeminal nerve that controls the feeling of touch, pain and pressure in the face. Nearly one-fourth of the people with acoustic neuroma report some amount of facial numbness i.e a loss of feeling or less frequently a weakness of the facial muscles. Facial numbness may also be reported in other problems like trigeminal neuralgia or growth of a tumor on the facial nerve.
Relatively less common symptoms of acoustic neuroma are:
- Frequent/persistent headache: This symptom may be reported in the case of a tumor that becomes large enough to block the flow of cerebrospinal fluid in the brain. The cerebrospinal fluid (CSF) surrounds the brain and spinal cord. It acts as a cushion to protect the delicate parts of the brain from any kind of chemical or physical insult. When the flow and drainage of CSF are obstructed, it can lead to an accumulation of fluid leading to a condition called hydrocephalus. The resultant increase in pressure and associated swelling starts compressing the brain within the skull. As a result, there is a headache which if left untreated may lead to brain damage.
- Earache: Pain in the ear is a relatively uncommon symptom that may be associated with many other underlying causes.
- Problems with vision: Even though it happens rarely, sometimes problems of vision due to hydrocephalus may be reported.
- Tiredness and lack of energy: Even though this is a nonspecific symptom, it can be reported sometimes with acoustic neuroma and is also associated with many causes.
How do doctors test and diagnose acoustic neuroma?
In case of a suspicion of an acoustic neuroma from the reported symptoms, your physician may refer you to an ear, nose and throat (ENT) specialist for further diagnosis and management.
After taking a thorough medical history and conducting a physical and ear examination, the following tests may be advised:
Hearing test i.e audiometry: The patient is made to hear sounds that are directed to one ear at a time. A range of sounds with varying tones and levels are directed towards the ear and patient’s response is recorded.
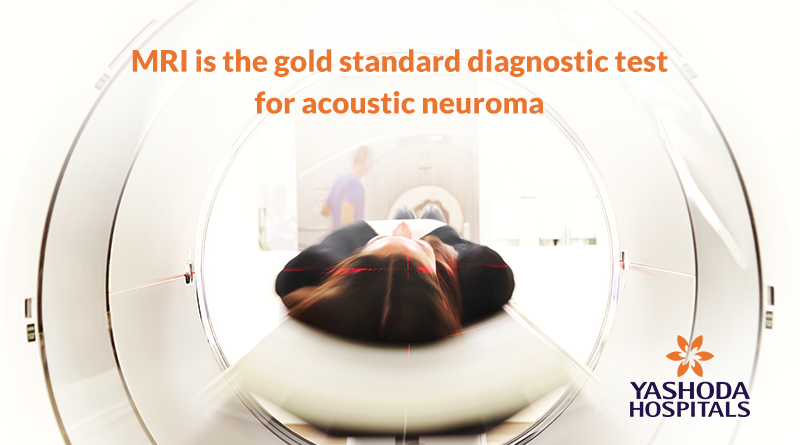
Imaging test: Magnetic resonance imaging (MRI) is one of the most preferred radiological imaging tests for diagnosing the presence of acoustic neuroma. It may be possible to identify small tumors even if 1 to 2 millimeters in diameter by this test. In case of unavailability or inability to perform MRI due to intolerance, computerized tomography (CT) may be used as an alternative. Sometimes temporal bone (CT) scans are necessary to reveal information about the bony canal.
What are the different treatments available for acoustic neuroma?
The treatment decisions for acoustic neuroma are usually based on:
- Size of the tumor and associated symptoms.
- Age and medical condition of the person.
Observation and monitoring: Sometimes in the case of very small-sized acoustic neuroma, your doctors may decide to just observe and monitor the tumor closely and periodically. This is so because of the nature of acoustic neuromas being slow-growing. Sometimes, they may not lead to any symptoms. Further, because acoustic neuromas are not cancerous and unlikely to spread, observation of small-sized tumors can be a safe option unless your doctor thinks otherwise. Because a surgical treatment has the possibility of developing complications and side-effects, your doctor will weigh the risks and benefits. In case your doctor decides to observe your condition, you may have to undergo scanning as and when advised.
Surgical treatment: In case of large-sized tumors with mass effect and brain stem distortion causing disturbing symptoms, surgery is a definitive treatment. Surgery is a procedure of choice for larger tumors and those which cause pressure symptoms.
For tumors less than 3 cm in size with an associated hearing loss, stereotactic radiosurgery is a preferred choice of treatment.
The factors that govern the suitability for surgery or radiotherapy include:
- Your age and general health that determines your fitness for undergoing surgery or radiotherapy
- Nature of the tumor: The size and location of your acoustic neuroma and its growth pattern will determine the type of treatment best recommended.
- The outcomes of the diagnostic test and scan can be used to decide the best treatment option for you.
Depending on the size of the tumor and its position on the acoustic nerve in the brain, surgery may be done either by a neurosurgeon or an ENT surgeon under general anesthesia.
Surgery/microsurgery is the most commonly advised treatment for acoustic neuroma. In about 95% of the cases, the tumors may be removed completely. In about 5% of cases, there may be a situation where a part of the tumor is left behind due to either a difficult location of the tumor or due to an underlying risk of damage to the nerve or another close by structures. In case a part of the tumor is left behind, it can be treated with radiotherapy.
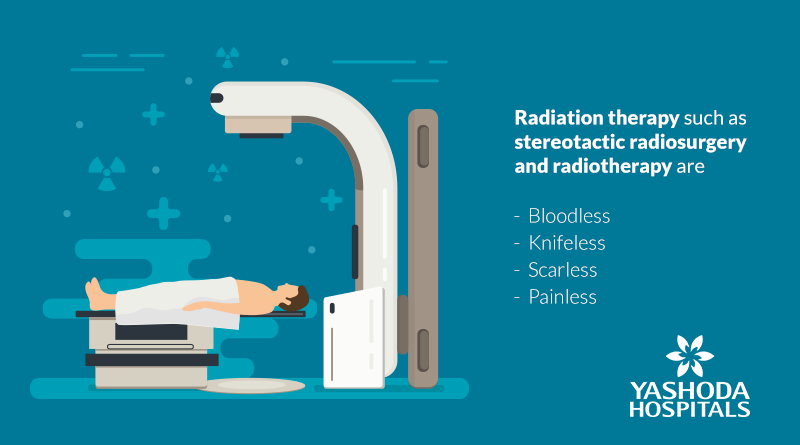
Stereotactic radiosurgery: This is an advanced treatment option that can be used for the removal of acoustic neuromas. Stereotactic radiosurgery consists of a procedure that involves delivery of radiation beam to a well-defined area where acoustic neuroma is located within the brain.
In this type of surgery, a point using three-dimensional (3D) coordinates is located in the acoustic neuroma tumor. A metal frame shaped like a halo is attached to the scalp of your head followed by a series of scans to determine the exact position of the tumor. Stereotactic radiosurgery is an advanced surgical treatment available only in a few large hospitals. The hospital should have the infrastructure support of both neurosurgery and oncology (cancer treatment) services for this surgery. One of the main advantages of stereotactic surgery is the prevention of any further growth and preservation of hearing function if intact at the time of surgery. The tumor, in this case, is eliminated by shrinkage.
Other modes of treatment may also include:
Stereotactic radiotherapy: A small dose of radiation is delivered to the tumor in several sessions with an intention to prevent the tumor from growing, without damaging the surrounding brain tissue.
Proton beam therapy: A type of radiation therapy that uses high-energy beams of positively charged particles called protons. A beam of protons is delivered to the tumor area in targeted doses to not only treat the tumors but also minimize exposure to radiation in the surrounding area.
Stereotactic Radiosurgery and Stereotactic Radiotherapy options are generally preferred in cases where:
- The patient is too old to undergo a surgery
- The patient is in a poor medical state and surgery is not a feasible option.
- Cases with residual tumors or tumors left behind after surgery
- Tumors which tend to recur i.e regrow after surgery
- Tumors which are large in size and cause additional symptoms due to the effect on neighboring structures known as “mass effect”
- Cases with some structural deformity like a distortion of the brain stem.
- Tumors with a size smaller than 3 cm accompanied with hearing loss.
The best course of treatment that should be undertaken depends on a multitude of factors and may vary from case to case. Hence it is recommended that a consultation with a neurosurgeon having expertise in such surgeries and who has an access to all state-of-the-art treatment options should be taken. It is an established fact that treatment outcomes are likely to be better in centers which not only have the right infrastructure but also have an integrated model of multidisciplinary care.
What are the possible complications of acoustic neuroma treatment?
Since acoustic neuroma occurs in a complex area of the brain, surgery for its removal is not devoid of the possibility of complications. Some of the possible complications include:
- Damage to the facial nerve, leading to palsy of the nerve: In case of large sized acoustic neuromas, sometimes during surgery, there may be a damage to the neighbouring facial nerve which controls the movements in the muscles of the face. This may lead to some degree of paralysis of a part of the face, leading to drooping of one side of the face.
- Damage to the acoustic nerve: Some degree of hearing loss is normally expected after treatment for acoustic neuroma.
- Damage to the trigeminal nerve: Similar to facial nerve, the trigeminal nerve is a neighbouring nerve responsible for sensations in the face. Due to the size of the tumor, an injury to this nerve during the surgery may lead to loss of sensation to some parts of the face.
As per the statistics from Acoustic Neuroma Association, in cases where radiosurgery is the treatment mode, there are 50 to 70 percent chances of preserving useful hearing with least risk or chance of permanent facial weakness. Further, it is also seen that radiosurgery can provide long-term tumor control in as high as 93 percent of cases.
What are the chances of survival after treatment for acoustic neuroma? What is the survival rate of acoustic neuroma?
The prognosis or outcome of acoustic neuroma is generally considered to be very good. Stereotactic radiosurgery has a low reported rate of serious complications with minimal mortality (death). These tumors respond well to treatment, complications are uncommon and chances of survival are extremely high. The most common side effect is often some hearing loss in the affected ear after treatment.
In cases with normal baseline hearing, up to 80% hearing can be preserved with surgery and nearly 60% to 80% of hearing can be preserved with radiation treatment. The outcome may, however, depend on the structure and size of the tumor, and surgical approach adopted. Treatment with contemporary or advanced methods is likely to have a very good prognosis with least possible chances of complications. From amongst the smaller sized tumors, nearly 40% to 60% may not require treatment. Tumors which have been treated with the focused radiation modality have a control rate as high as >90%.
How long does it take to recover after treatment for acoustic neuroma?
Once the surgery for acoustic neuroma is done, you will have to remain hospitalized for a few days for monitoring your recovery. It usually takes 6-12 weeks for recovery after discharge. Generally, no further treatment may be required in case of a completely removed tumor.
Stereotactic radiosurgery is a day care procedure and recovery is very rapid. There is no pain or risk of infection associated with this procedure. Thus, the patient leaves the hospital on the same day, although follow-up imaging and retreatment may be necessary in some cases.
It is generally seen that less than 5% of acoustic neuromas recur, which is more likely in cases of NF2. Once the treatment is completed for acoustic neuroma you may be required to be followed up in the outpatient department for assessment of any symptoms or signs of it recurring.
References:
Mayo Clinic. Acoustic Neuroma. Available at: https://www.mayoclinic.org/diseases-conditions/acoustic-neuroma/symptoms-causes/syc-20356127. Accessed on July’ 14, 2018.
US National Library of Medicine. Acoustic Neuroma. Available at: https://medlineplus.gov/acousticneuroma.html. Accessed on July’ 14, 2018
Cedars-Sinai. Acoustic Neuroma. Available at:http://www.braintumortreatment.com/Brain-Tumors/Tumor-Types/Acoustic-Neuroma.aspx. Accessed on July’ 14, 2018
Reports Healthcare. Acoustic Neuroma –Everything you should know. Available at https://reportshealthcare.com/acoustic-neuroma-everything-you-should-know/. Accessed on July’ 14, 2018
Epocrates. Acoustic Neuroma. Available at. https://online.epocrates.com/diseases/73151/Acoustic-neuroma/Prognosis. Accessed on July’ 14, 2018
About Author –
Dr. Ravi Suman Reddy, Senior Neuro & Spine surgeon, Yashoda Hospitals – Somajiguda
MCH (NIMHANS), Advanced training in Stereotactic Radiosurgery (Brain Lab Academy – Germany). His expertise includes frameless stereotactic neurosurgery, minimally invasive spine surgery, spine stabilization, nerve radiofrequency ablation, cranial micro neurosurgery, cranio-spinal trauma, and endoscopic surgery.



 Appointment
Appointment Second Opinion
Second Opinion WhatsApp
WhatsApp Call
Call More
More






{kind=link}